


It’s a cold, drippy February afternoon. I’m ensconced in what I’ve come to call my “nest,” a spot on the living room sofa where I spend much of the two-ish days after each treatment when I feel sluggish and sad. Something about this chemotherapy drug, or the several side-effects-mitigators administered alongside it, sends my mood plunging along with my energy the second and third days post-infusion. I’ve tried to learn to roll with it, give myself permission to rest, curl up with a blanket and a good book for distraction. Yet I often feel guilty and antsy, frustrated by my lack of focus and inability to will myself out of my funk.

It’s fecund breeding ground for brooding, and today my thoughts are vacillating between “the human body is a strange and wondrous organism” and “what fresh hell is this?” To wit: I’ve been dealing with persistent hoarseness going on two months now, and on Tuesday I saw an ear, nose, and throat specialist to see if we could get at the root of the problem. I’ve also been having issues with swallowing, and in the past year have undergone repeated endoscopic dilations, the last one just a few weeks ago. My hoarseness mysteriously disappeared for two days right after the latest endoscopy, but then returned. On the morning of my ENT appointment, I almost choked on a vitamin tablet. It all seemed like it must be connected, somehow.
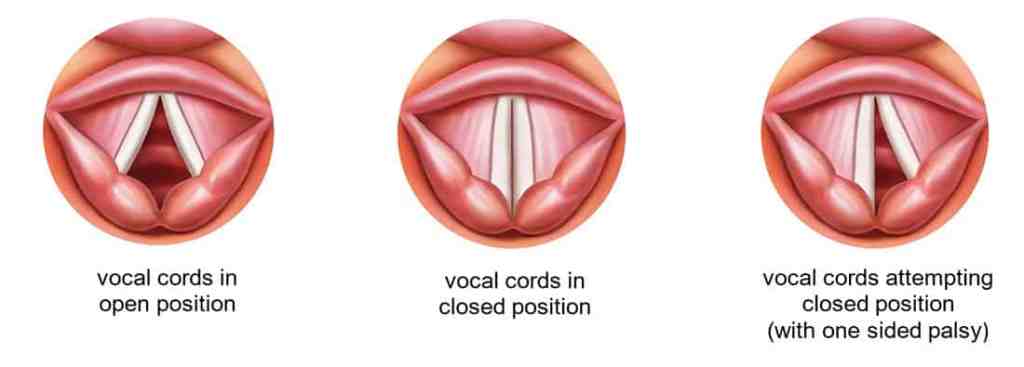
After listening to me describe my history, the ENT doctor asked if I’d had a recent CT scan of my chest, and “whether it showed any mediastinal lymphadenopathy.” Translation: enlarged lymph nodes in the chest. He suspected that my left vocal cord was paralyzed, possibly a result of enlarged lymph nodes pressing on the recurrent laryngeal nerve, which loops down under the rib-cage. I was surprised that a problem with the lymphatics in my chest could be responsible for issues in my throat, but it’s not the strangest detour my body has taken along this path. A paralyzed vocal cord would explain the hoarseness as well as the swallowing issues, since the vocal cords close during swallowing as well as speaking. If folds on either the left or right are paralyzed, the resulting gap can cause vocal changes and aspiration. Who knew?
The doctor showed me a diagram of what my larynx should look like in both its open and closed positions, then threaded a tiny camera attached to a long, flexible tube through my right nostril and into my sinus cavity so he could take a look at my larynx—uncomfortable, but not much worse than a Covid test. He situated the screen so I could see the camera feed, too, and there it was–my voice box. He asked me to say “eeeeeee,” and while the right side of my larynx flexed closed, the left side only moved a tiny bit toward the center, leaving a sliver of open space in the middle.
It was strangely satisfying, after so many years of scans and biopsies with days or weeks of lag time between test and diagnosis, to see and identify the problem so quickly and definitively. I’m trying not to be too anxious about possible underlying causes for the paralysis. My November CT showed the cancerous mediastinal lymph nodes had shrunk since the previous scan; it is a bit concerning that they may have enlarged again, although inflammation could be a result of a robust immune response. It’s also possible, given my history of radiation and the fibrosis that has developed, that one or both of those have injured the recurrent laryngeal nerve; injury can also occur during endotracheal intubation, which I’ve had my fair share of in the past year.
The treatment for a paralyzed vocal cord is a bit less straightforward than diagnosis, although sometimes the problem simply resolves itself over time. Medically, the impact on swallowing is considered more urgent than vocal changes, so I’ll undergo a “swallowing study,” which as best I understand is me swallowing a series of barium-infused substances of different consistencies while they x-ray the process. Yum. I’ve also been referred to a voice doctor. The likely treatment is injection into the cord of a filler similar to those used in cosmetic procedures to plump it up. For someone who doesn’t like a lot of stuff happening around her throat, the prospect of this procedure both fascinates and horrifies me.

Dealing with a chronic illness means you get all kinds of anatomy lessons you never anticipated (or wanted), many of which fall into the “stuff I never knew could happen” and “wow, bodies sure are weird” categories. I’ve always loved learning new things, so I’ve tried to embrace my innate curiosity, use it as a kind of coping mechanism. That’s more challenging some days than others. Still, whether it tracks the emergence of a new virus or the development of the vaccine that tames it, the science of life astounds. One might as well be amazed.
Inside, I hunker down into my nest, cup of hot tea in hand. Outside, the rain has shifted to sleet. Ice coats the trees, lacquering their black satin branches. They shine against a gray flannel sky.






